基于时机理论的赋能健康教育对病毒性肝炎患者服药依从性及自护能力的影响
作者: 冯翠 张娜
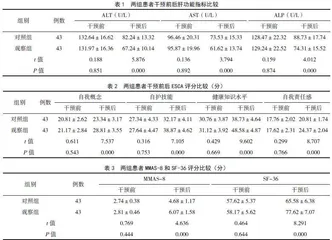
【摘要】 目的 探讨基于时机理论的赋能健康教育对病毒性肝炎患者服药依从性及自护能力的影响。方法 选取2022年1月- 2023年1月医院收治的86例病毒性肝炎患者为研究对象,依据组间性别、年龄等基线资料均衡可比的原则,采用随机数字表法分为对照组和观察组,每组43例。对照组给予常规健康教育干预,观察组给予基于时机理论的赋能健康教育干预;两组均干预至患者出院3个月。对比两组患者干预前后肝功能[丙氨酸转氨酶(ALT)、天冬氨酸转氨酶(AST)、碱性磷酸酶(ALP)]变化、服药依从性[Morisky服药依从性量表(MMAS-8)]、自护能力[自我护理能力量表(ESCA)]及生活质量(SF-36)评分。结果 赋能健康教育干预前,两组患者ALT、AST及ALP水平比较差异无统计学意义(P>0.05);干预后,观察组患者ALT、AST及ALP水平低于对照组,差异有统计学意义(P<0.05)。赋能健康教育干预前,两组患者自我概念、自护技能、健康知识水平、自我责任感等ESCA各项评分比较差异无统计学意义(P>0.05);干预后,观察组患者自我概念、自护技能、健康知识水平、自我责任感等ESCA评分高于对照组,差异有统计学意义(P<0.05)。赋能健康教育干预前,两组患MMAS-8和SF-36评分比较差异无统计学意义(P>0.05);干预后,观察组患者MMAS-8和SF-36评分高于对照组,差异有统计学意义(P<0.05)。结论 将基于时机理论的赋能健康教育应用于病毒性肝炎患者,可以改善患者肝功能,提高患者服药依从性及自护能力,提升患者生活质量。
【关键词】 时机理论;赋能健康教育;病毒性肝炎;服药依从性;自护能力
中图分类号 R47 文献标识码 A 文章编号 1671-0223(2025)03--05
Effect of empowering health education based on timing theory on medication adherence and self-care ability of patients with viral hepatitis Feng Cui, Zhang Na. Department of Hepatology,Tai'an 88 Hospital, Tai'an 271000,China
【Abstract】 Objective To explore the impact of timing theory based empowering health education on medication adherence and self-care ability in patients with viral hepatitis. Methods Using convenience sampling method,86 patients with viral hepatitis admitted to the hospital from January 2022 to January 2023 as the research subjects. According to the principle of balance and comparability of baseline data such as gender and age between groups, they were divided a control group and an observation group using a random number table method, with 43 cases in each group. The control group received routine health education intervention until 3 months after the patients were discharged, while the observation group received health education intervention based on the theory of empowerment until 3 months after the patients were discharged.The changes in liver function [alanine aminotransferase (ALT), aspartate aminotransferase (AST),alkaline phosphatase(ALP)], medication adherence [Morisky medication adherence scale-8 items(MMAS-8)], exercise of self-care agency scale (ESCA) and and quality of life (SF-36) before and after the intervention were compared between the two groups. Results Before the health education intervention, there were no significant differences in the levels of ALT, AST, and ALP between the two groups(P>0.05);after the intervention, the levels of ALT, AST, and ALP in the observation group were lower than those in the control group, and the differences were statistically significant (P<0.05).Before the health education intervention, there were no significant differences in the ESCA scores of self-concept, self-care skills, health knowledge level and self-responsibility between the two groups(P>0.05);after the intervention, the ESCA scores of self-concept, self skills, health knowledge level, and self-responsibility in the observation group were higher than those in the control group, and the differences were statistically significant (P<0.05).Before the intervention of health education empowerment, there was no significant difference in MMAS-8 and SF-36 scores between the two groups (P>0.05); after the intervention, the MMAS-8 and SF-36 scores in the observation group were higher than those in the control, and the difference was statistically significant (P<0.05).Conclusion Applying empowerment health education based on timing theory to patients with viral hepatitis can improve the patients'liver function levels, enhance their medication adherence and self ability, and improve their quality of life.
【Key words】 Timing theory; Empowering health education; Viral hepatitis; Medication compliance; Self care ability
病毒性肝炎主要有甲、乙、丙、丁、戊5种类型,具有高传染性,患者常出现食欲减退、恶心和上腹部不适等症状[1]。2019年全球慢性乙型病毒性肝炎感染者有2.96亿,慢性丙型病毒性肝炎感染者5800万[2]。我国病毒性肝炎的防治意识普遍不足,患者不能及时发现感染并就医,从而延误治疗,导致病情加重。随着病情恶化,病毒对肝脏的侵袭加重,导致并发症和病死率增加[3]。因此,提高病毒性肝炎患者对疾病的认识,加强预防意识至关重要。健康教育发挥着至关重要的作用,可以提高患者对疾病的认知水平,促进其健康行为改变。但常规健康教育缺乏个性化和情感支持。而赋能健康教育强调个体的自我决定和自我效能感,能更好地帮助个体树立自信心,应对疾病挑战[4]。时机理论提供理解和干预健康行为的框架,指导人们在特定时机下做出决策和行为改变,通过识别和利用这些时机可以更有效地推动健康行为的发生和持续[5]。基于此,本研究探讨基于时机理论的赋能健康教育对病毒性肝炎患者服药依从性及自护能力的影响。
1 对象与方法
1.1 研究对象
选取2022年1月- 2023年1月医院收治的86例病毒性肝炎患者为研究对象。纳入标准:①符合《病毒性肝炎健康管理专家共识(2021年)》[6]中病毒性肝炎诊断标准;②经实验室检查确诊病毒性肝炎;③年龄>18岁。排除标准:①合并其他传染性疾病者;②合并严重肝脏疾病者;③疾病已进展至肝硬化者。依据组间基线资料均衡可比的原则,采用随机数字表法分为对照组和观察组,每组43例。对照组男26例,女17例,年龄32~71岁,平均年龄43.16±4.47岁;病原学分型:甲型13例、乙型19例、丙型11例。观察组男28例,女15例,年龄30~70岁,平均年龄42.87±4.32岁;病原学分型:甲型11例、乙型22例、丙型10例。两组患者上述基线资料比较差异无统计学意义(P>0.05),具有可比性。本研究通过医院伦理委员会批准,患者均签署知情同意书。
1.2 健康教育方法
1.2.1 对照组 给予患者常规健康教育干预至出院3个月,向患者介绍疾病的基本情况、治疗过程以及疾病转归等。提供用药手册及准则,以便患者更好地了解其所使用药物的相关信息,并且按照医嘱正确服用药物。同时,对患者进行心理指导,帮助患者调整情绪,增强其应对疾病的信心和勇气。
1.2.2 观察组 给予患者基于时机理论的赋能健康教育干预至出院3个月。首先成立干预小组,由1名护士长及3名专科护士组成,护士长担任组长。实施前进行统一培训,包括病毒性肝炎知识、时机理论相关内容、赋能教育理论及沟通技巧、如何处理患者心理问题等。小组讨论制定赋能教育干预方案,进行小组讨论,每周1次,评估效果并改进。干预时机划分为确诊期(疾病发生到明确诊断)、治疗期(决定治疗至病情稳定)、出院准备期(出院前1天至出院)、适应期(出院后至3个月)。具体实施内容如下。
(1)确诊期:向患者介绍病毒性肝炎的病因、传播途径、病程发展等基本知识,包括早期症状如乏力、食欲减退、黄疸等,以及采取的治疗措施,告知患者出现任何情况都应该及时就医,了解诊断检查方法,如血清学检查、核酸检测等,同时提供心理支持,帮助患者应对焦虑、恐惧情绪。
(2)治疗期:在患者入院6h内,干预小组查阅患者病历,并与患者进行面对面访谈,确定患者当前面临的主要问题,并鼓励其表达内心的情感和感受。在入院第3天,医护人员将进行第2次访谈,以进一步了解患者的情况和感受。随后每3~5天进行一次面对面指导,每次20min,直至患者出院。在面对面的交流中,干预小组与患者一同设立治疗目标,涉及饮食、药物、日常生活等方面的计划,并向患者强调抗病毒治疗的重要性。干预小组确定护理问题、目标和计划,打印清单并挂于患者床尾,使其知晓并配合医护实现计划。小组协助患者完成目标,达成后在床头计划单上签字,增强其信心。
(3)出院准备期:干预小组针对已完成或未完成的目标给予反馈和指导,制定延续性护理方案,个性化地调整护理方案,随访沟通。
(4)适应期:向患者发放自我管理监控卡,每周与患者进行一次电话随访,了解患者自我管理情况,并针对不足之处进行调整。同时,鼓励家属积极参与到患者的治疗管理环节中,包括监督患者服药、协助应对用药不良反应等。
1.3 观察指标
(1)肝功能:采用生化分析仪检测丙氨酸转氨酶(alanine aminotransferase,ALT)、天冬氨酸转氨酶(aspartate aminotransferase,AST)、碱性磷酸酶(alkaline phosphatase,ALP)水平。
(2)自护能力:采用自我护理能力量表(exercise of self-care agency scale,ESCA)[7]评估患者自我护理能力,该量表包括自我概念(9项条目)、自护技能(12项条目)、健康知识水平(14项条目)、自我责任感(8项条目)4个维度,共43项条目,每项条目0~4分,得分越高提示自我护理能力越好。
(3)服药依从性:采用Morisky服药依从性量表(Morisky medication adherence scale-8 items,MMAS-8)[8]评价患者服药依从性,共8个问题,总分8分,分值越高表明服药依从性越好。
(4)生活质量:采用健康调查简表(the MOS item short from health surv,SF-36)[9]评估患者的生活质量,从情感职能、生命活力、总体健康等8个维度进行评估,共36个条目,总分100分,评分越高表示生活质量越好。